Our arteries deteriorate with age. Autopsy studies of younger people who died from accidents, homicide, and other non-cardiac causes demonstrate that the process of atherosclerosis begins in the 20’s as a “fatty streak.” By the time a person has a myocardial infarction (heart attack) in his or her 50’s, the process has quietly gone unnoticed for decades. I like to say that atherosclerosis doesn’t cause symptoms…..until it does. At least 25% of patients who experienced a myocardial infarction had no previous symptoms.
I like to discuss this issue with younger patients, with the hope of starting lipid-lowering measures to reduce apoB and LDL cholesterol at a young age. Unsurprisingly, I often get push-back from my younger patients when I suggest pharmacotherapy.
Despite living in a wealthy country, we are becoming sicker. Coronary artery disease is the #1 cause of death in the US and the world at large, and the US death rate from coronary artery disease is the second highest among 17 peer countries.
Risk factors for coronary artery disease include family history, dyslipidemia (high LDL-cholesterol, high Lp(a), and apoB), obesity, sedentary lifestyle, insulin resistance, type 2 diabetes, hypertension, and cigarette smoking. Men develop coronary artery disease 10 years before women.
It can be difficult to accurately determine whether an individual has vascular disease based on patient history alone.
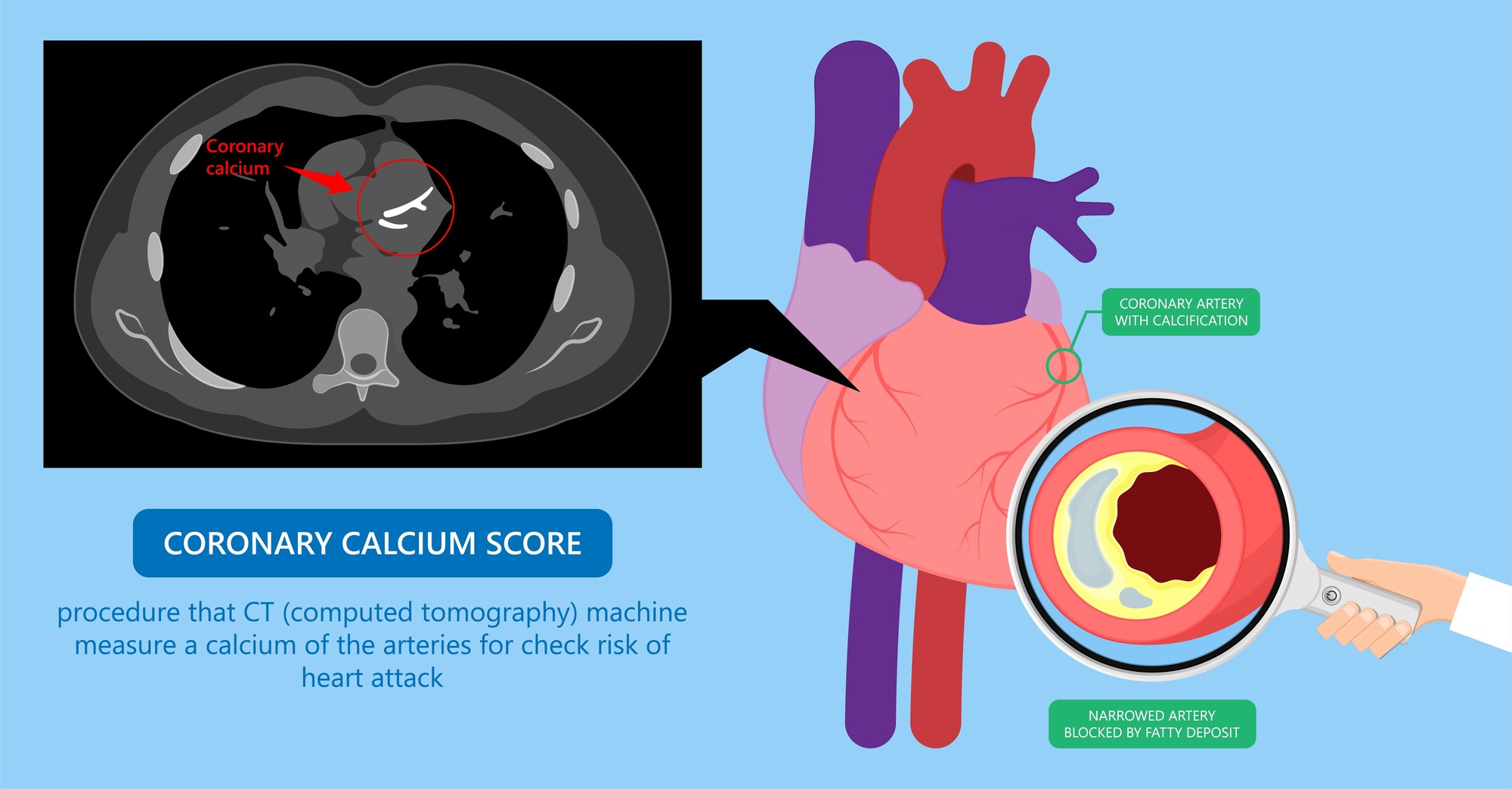
With age, coronary artery lesions, which begin as soft plaques, become calcified and are easily visible on CT of the chest.
A coronary artery calcium scan is an inexpensive (around $200) CT of the chest that employs low dose radiation and does not require IV contrast. The scan is less accurate for people below 40 years of age, since coronary artery plaques in younger people are more likely to be soft and non-calcified, making them less likely to be visible on a CT scan.
The degree of calcification within the coronary arteries is quantified by the Agatston and volume scores. These scores are compared with your age and gender matched peers. A higher score correlates with higher burden of coronary artery disease and future risk of infarction. Coronary artery calcification is a sign to practice assertive measures to prevent progression of plaque and reduce the risk of infarction.
The degree of calcification within the coronary arteries is quantified by the Agatston and volume scores. These scores are compared with your age and gender matched peers. A higher score correlates with higher burden of CAD and future risk of infarction. Coronary artery calcification is a sign to practice assertive measures to prevent progression of plaque and reduce the risk of infarction.
Agatston coronary artery calcium scoring
CAC – coronary artery calcium
| CAC score (Agatston method) | Risk analysis | Clinical correlation |
| 0 | Absent/ No risk | Low risk of future cardiovascular events. |
| 1-10 | Minimal | Minimal atherosclerosis may be present with a low risk of future cardiovascular events. |
| 11-100 | Mild | There is likely mild to minimum coronary artery stenosis. A mild risk of coronary artery disease exists. |
| 101-400 | Moderate | Reasonable amount of plaque can be confirmed. Has a moderately increased risk of future cardiovascular events. |
| >400 | High | A high coronary calcium score corelated with a significant risk of having a cardiovascular event (such as myocardial ischemia) in near future. |
The coronary artery calcium scan is best used for people who are not currently experiencing chest discomfort and are thought to be at low to intermediate risk of developing symptomatic CAD. It is not meant for people at high-risk of CAD; in these patients, I would recommend proceeding directly to pharmacotherapy to reduce apoB and LDL cholesterol, in addition to treating other risks such as hypertension and so on.
I typically send a patient with a high coronary artery calcium score (400 or more) to a Cardiologist for a cardiac stress test to rule out obstruction within the artery.
If a patient has increased risks for CAD but has a zero or low calcium score and does not wish to intitate pharmacotherapy, I recommend rescanning in 3 years to see if the score increases.