Insulin resistance is a very common metabolic abnormality due to a combination of genetics, a change in our dietary habits, and overconsumption of calories. The incidence of insulin resistance is rising steadily in this country along with the increasing incidence of obesity. Not all patients with insulin resistance are overweight or obese.
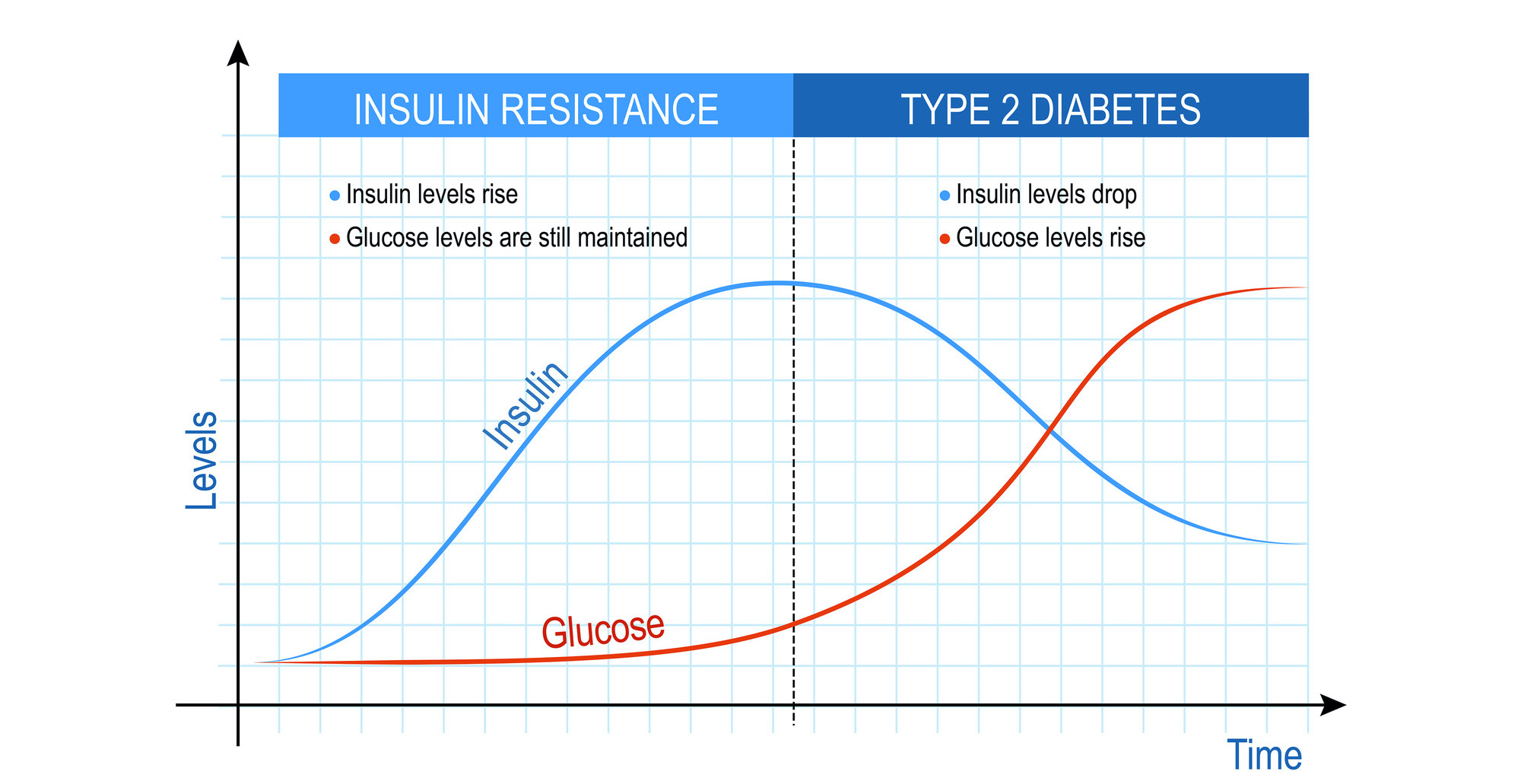
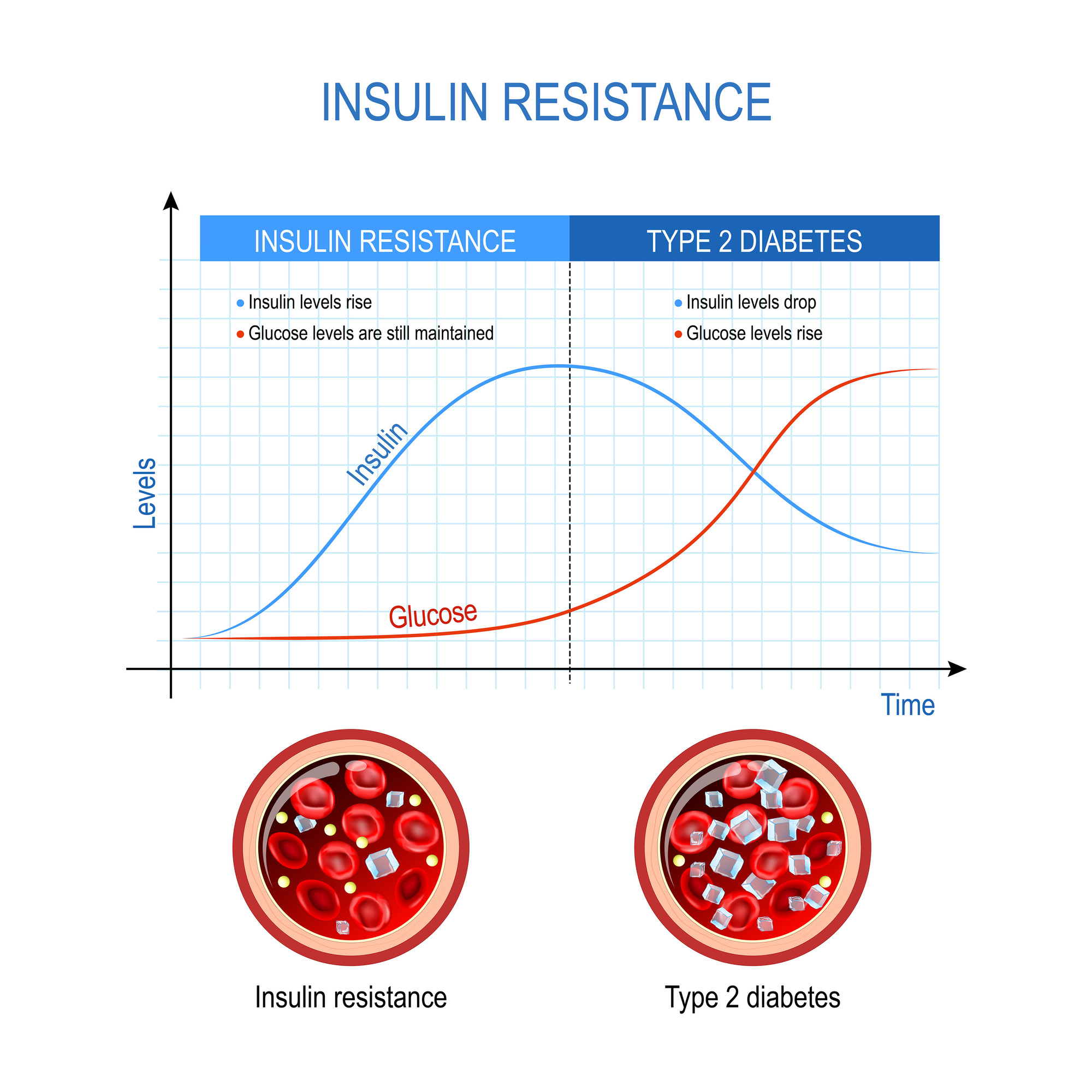
After a meal, the pancreas senses the rise in blood glucose and produces insulin to drive glucose in the cells where it is used for fuel. Once insulin attaches to its receptor on the cell surface, glucose transport tubes called glut4 migrate to the cell surface, where they allow glucose to pass into the cell. However, with insulin resistance, the cells ignore the signal of insulin, and the glu4 tubes are prevented from migrating to the cell surface, causing reduced passage of glucose into cells. The result is that the blood level of glucose rises. This causes a domino effect of different problems.
The pancreas, recognizing that the level of insulin is not sufficient to pass glucose into the cells, increases insulin secretion. A patient with insulin resistance typically has an elevated insulin level. This in turn, increases secretion of a hormone called IGF-1, and there is a strong association between IGF-1 and cancer. People with insulin resistance have a significantly increased risk of cancer.
An elevated insulin level reduces lipolysis (the breakdown of triglycerides, which is another name for fat molecules). This causes accumulation of fat within organs and muscle. Patients with insulin resistance will often have a high blood level of triglycerides (normal physiologic triglycerides are 30-70, not less than 150 as most labs would suggest), low HDL cholesterol, and high apolipoprotein B (also known as apoB).
To explain how insulin resistance increases the risk of vascular (artery) disease, I will briefly explain cholesterol transport. Lipoproteins transport cholesterol and triglycerides through the bloodstream (think of a FedEx van). The lipoproteins are produced in the liver, and are released into the bloodstream to deliver cholesterol and triglycerides to various tissues. The lipoproteins are meant to return to the liver for recycling. However, there are 3 types of lipoproteins that can pass into the artery lining and become trapped like a lobster in a cage. When the lipoproteins, laden with cholesterol, become oxidized, they attract inflammatory cells of the immune system, setting up a chronic, destructive inflammation, ultimately damaging the lining to cause atherosclerosis. The 3 atherogenic lipoproteins include LDL, VLDL, and Lp(a). Each lipoprotein has one molecule of apoB on the surface. While insulin resistance does not alter the amount of cholesterol within a given amount of blood, it causes of redistribution of cholesterol within them such that they become more numerous. Evidence is clear that a higher number of lipoproteins, independent of the amount of cholesterol they carry, is a strong risk factor for vascular disease (if you have more numerous lipoproteins, more of them will pass into the artery lining – this is called gradient pressure). Because there is one apoB molecule on every atherogenic lipoprotein, apoB allows us to calculate the number of atherogenic proteins to assess your risk.
The visceral fat (the fat contained within the organs such as liver, pancreas, and so on) releases inflammatory chemicals such as IL-6 and TNF to cause widespread inflammation. I often see elevated inflammatory markers on blood testing of obese patients with insulin resistance. Insulin resistance is correlated with increased risk of coronary artery disease and dementia.
When fat accumulates in the liver, the condition is called hepatic steatosis. Over time, this can lead to chronic liver disease. Hepatic steatosis is reversible with better diet, lower in calories and carbohydrates, regular and vigorous exercise (zone 2), and weight loss.
Recommendations
Consume only 2 meals daily separated by 8 hours, such as lunch and dinner; this mainly reduces your calorie consumption over 24 hours
Lower consumption of total calories and carbohydrates, such as starchy food, including bread, pasta, rice, and noodles
Protein is satiating, I recommend you consume at least 1 gram of protein per kilogram of body weight per day
If you need to snack, I suggest popcorn or nuts rather than processed snacks such as chips
Lower consumption of processed foods in which fiber has been stripped
Consume a diet high in vegetables; fiber feeds your colon microbiome, which improves glucose metabolism
Exercise as often as possible, make it a priority in your weekly schedule
If you are struggling to lose weight, consider pharmacotherapy with a GLP-1 agonist such as Ozempic or other to increase satiety.